Dengue fever case
General Medicine E-log
60 year old male presented to the OPD with fever and giddiness since 3 days.
Chief complaints:
Patient (60, M) who is a farmer by occupation came to the casualty with chief complaints of fever and giddiness for the past 3 days.
History of present illness:
Patient was apparently asymptomatic 3 days back when he developed giddiness and fever which was of sudden onset and continuous nature. It was not associated with chills or rigor. No diurnal variations in fever were observed.
He also complained of loss of taste.
However, he had no complaints of:
No C/O - cold or cough.
No C/O - abdominal pain, nausea, loose stools or vomiting.
No C/O - burning micturition, decreased urine output, pedal edema or facial puffiness.
No C/O - chest pain, palpitations, or syncopal attacks.
No C/O - SOB, orthopnea or PND.Past history:
He is not a known case of HTN, DM, CAD, CVA, Epilepsy, TB, Asthma or Thyroid disorders.
He is not a known case of HTN, DM, CAD, CVA, Epilepsy, TB, Asthma or Thyroid disorders.
Personal history:
Occupation: farmer
Occupation: farmer
Diet: mixed
Appetite: decreased
Sleep: adequate
Bowel and bladder habits: regular
Addictions: he consumes toddy occasionally.
No known drug allergies.
Appetite: decreased
Sleep: adequate
Bowel and bladder habits: regular
Addictions: he consumes toddy occasionally.
No known drug allergies.
Family history:
No significant family history.
No significant family history.
General examination:
Patient is conscious, coherent and co-operative.
Mild pallor is present.
No icterus, cyanosis, clubbing, koilonychia, generalized lymphadenopathy, edema is seen.
Vitals:
BP: 100/60
Temperature: 95.7°F
PR: 46 bpm
PR: 46 bpm
SpO2: 95% (at room air)
GRBS: 218 mg/dl
GRBS: 218 mg/dl
Systemic Examination:
CNS:
Speech: normal
No signs of meningeal irritation
Motor & sensory system: normal
Cranial nerves: intact
Speech: normal
No signs of meningeal irritation
Motor & sensory system: normal
Cranial nerves: intact
Reflexes: present
Right Left
Biceps: 2+ 2+
Triceps: 2+ 2+
Supinator: 2+ 2+
Knee: 2+ 2+
Ankle: 2+ 2+
CVS:
S1, S2 were heard
No Murmurs
No thrills
Respiratory system:
Position of Trachea: central
BAE: present
NVBS heard
No added sounds
Per Abdomen:
Soft, non tender
Hernial orifices are normal
No palpable masses
Bowel sounds heard
No thrills
Respiratory system:
Position of Trachea: central
BAE: present
NVBS heard
No added sounds
Per Abdomen:
Soft, non tender
Hernial orifices are normal
No palpable masses
Bowel sounds heard
Provisional diagnosis:
Pyrexia under evaluation.
Investigations:
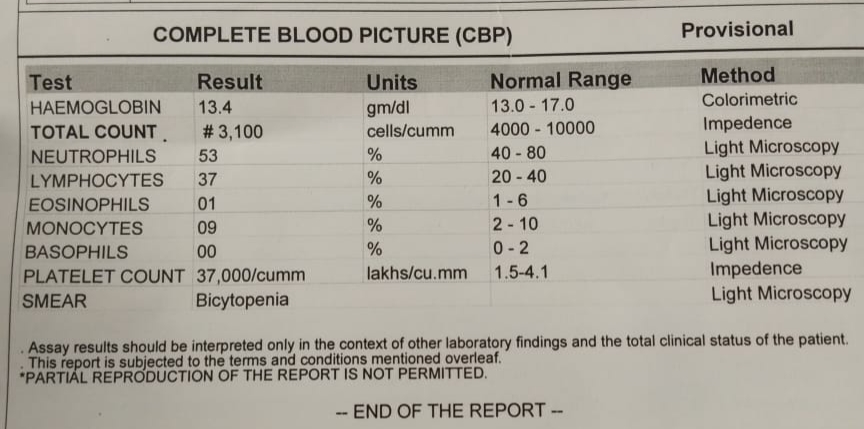
CBP
6/07/21
Blood parasites
6/07/21

Prothrombin time (PT)
6/07/21

Activated partial thromboplastin time (APTT)
6/07/21

Dengue NS1 Antigen Rapid Test
6/07/21

Note: test results to be confirmed by ELISA.
Complete urine examination
6/07/21

Haemogram
6/07/21

7/07/21

9/07/21

10/07/21

Fever chart
(Updated: 9/07/21)

ECG
6/07/21

Rate: 41 bradycardia (could be sinus bradycardia)
Rhythm: regular
P wave: present, indicates impulse originating above the ventricles (SA node, atria)
QRS complex duration: normal
PR, QT interval duration: normal
T wave: normal
Final diagnosis:
Dengue fever with thrombocytopenia.
Treatment given (present course in the hospital):
6/07/21
1. IV fluids 20 NS/20 RL at 25ml/hr.
2. Tab. PCM 650mg PO/ TID
3. Inj. PCM 1g/iv/stat, (if temperature is more than 101°F).
4. Inj. PAN 40mg IV/OD
5. Inj. Optineuron 1amp in 100ml NS/IV/OD
2. Tab. PCM 650mg PO/ TID
3. Inj. PCM 1g/iv/stat, (if temperature is more than 101°F).
4. Inj. PAN 40mg IV/OD
5. Inj. Optineuron 1amp in 100ml NS/IV/OD
6. BP, PR, RR and SpO2 charting 4th hourly.
7/07/21
1. IV fluids 20 NS/20 RL at 25ml/hr
2. Tab. PCM 650mg PO/ TID
3. Inj. PCM 1g/iv/stat, (if temperature is more than 101°F).
4. Inj. PAN 40mg IV/OD
5. Inj. Optineuron 1amp in 100ml NS/IV/OD
3. Inj. PCM 1g/iv/stat, (if temperature is more than 101°F).
4. Inj. PAN 40mg IV/OD
5. Inj. Optineuron 1amp in 100ml NS/IV/OD
6. BP, PR, RR and SpO2 charting 4th hourly.
8/07/21
1. IV fluids 20 NS/20 RL at 25ml/hr
2. Tab. PCM 650mg PO/ TID
3. Inj. PCM 1g/iv/stat, (if temperature is more than 101°F).
4. Inj. PAN 40mg IV/OD
5. Inj. Optineuron 1amp in 100ml NS/IV/OD
2. Tab. PCM 650mg PO/ TID
3. Inj. PCM 1g/iv/stat, (if temperature is more than 101°F).
4. Inj. PAN 40mg IV/OD
5. Inj. Optineuron 1amp in 100ml NS/IV/OD
6. BP, PR, RR and SpO2 charting 4th hourly.
Advice at discharge:
1. Tab. PCM 650mg PO/TID
2. MVT Tab * 15 days
3. Plenty of oral fluids
Discussion (queries):
1) How is dengue transmitted?
The virus is transmitted to humans through insect vectors - bite of female mosquitoes of Ades aegypti species. Maternal transmission (from infected pregnant mother to fetus) of the virus is possible too.
2) What is the cause for thrombocytopenia in dengue?
Platelet consumption is increased due to ongoing coagulopathy process, activation of complement system and peripheral sequestration.
There is decreased production caused by infection induced bone marrow suppression which may even lead to bi or pancytopenia.
More about Dengue fever:
Thank you for reading.


Comments
Post a Comment